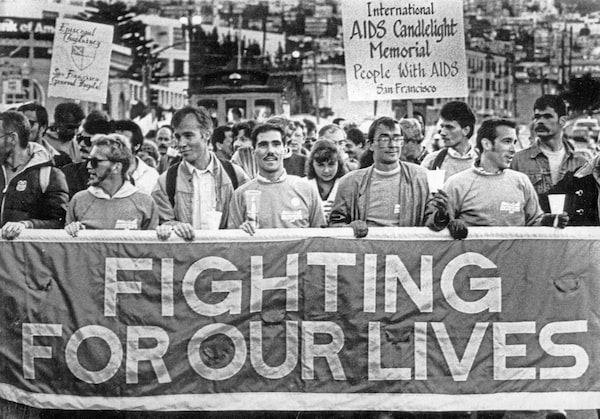
An estimated 5,000 marched in the annual AIDS candlelight march seen here on May 26, 1986.John Green/UPI
John MacLeod is a primary-care physician with 30 years of experience in HIV care.
Being a gay man in the 1980s was terrifying enough. Homophobia was pervasive at the time, and coming out came with substantial risks – including the threat of rejection and violence. This was a time before human-rights protections for gays. Many lived silently in shame.
When I started medical school in 1982, reports of gay men dying from an unknown illness started to appear in the news. HIV and I both came out in the early 1980s, and so my future path would be paved by an epidemic.
For years, I lost many close friends and patients. These were not occasional deaths; they were numerous and part of my everyday life. I grieved each and every loss. And as a gay man, I knew I was vulnerable.
A phone call from my first love changed the course of my life: He had tested positive for HIV. With no treatment options, I saw nothing positive nor helpful in being tested. My boyfriend died after my first year of practice. We were both 30 years of age.
Our medical system was unprepared for what unfolded. There was panic in everyday life, and it was common for people to die in isolation. I watched men die without the comfort of their own families, and I saw young women blamed and ostracized because of the shame that came with being infected with HIV. The effects of stigmatization were profoundly evident all around me, in both my professional life and my personal life.
Today, I am faced with a new viral epidemic, yet much of what is unfolding is similar to what I saw in the early years of HIV. I’m self-isolating at home this week, short of breath with heaviness in my chest. It is not clear if this is from COVID-19, but this is the first of many unknowns. I am aware that as a physician I am at a higher risk and I will undoubtedly see more deaths and illnesses over the coming months, something that still haunts me from my early years in HIV care. And just last week, U.S. President Donald Trump announced he’s halting funding to the World Health Organization, a blow to the collective effort we learned that we needed to face HIV.
Now, as I recover, I’m left to consider this question: Why weren’t we better prepared this time?

Alan Shaw, left, and Robert Hilfrety share a tender moment outside of the Fifth International Conference on AIDS in Montreal on June 6, 1989.PIOTR ANDREWS/The Globe and Mail
I first became familiar with how infectious diseases can change lives at the age of five, when my great aunt returned home after her retirement. She was a kind and gentle woman who showered me with attention, and she told me stories from her life – including from the years she spent convalescing in a tuberculosis sanatorium shortly after finishing teachers college. The disease had intruded on her most productive years, when she likely would have married and had children of her own. I often reflect on what her life must have been like, moved into a sanatorium away from her community and life. I think about her reality of stigmatization and social isolation, ostracized with no available effective treatment at the time. I had no idea that the stories she shared with me would foreshadow my own experience with a different infectious disease.
My great aunt remains an enduring reminder for me that pandemics are not new in human history. Infectious diseases have historically come in waves. The American plagues of the 16th century were a cluster of diseases brought to this continent by European explorers, an example of the contribution of globalization in the spread of disease. Similarly, the flu epidemic of 1889 occurred during the industrial age, when new transport links made it easier for the flu virus to span the globe. The Spanish flu of 1918-19 infected 500 million people, one-third of the world’s population at the time. Much like influenza, COVID-19 favours crowds of people in close contact.
Although there are differences between COVID-19 and HIV, the ways the viruses spread through our communities are in many ways similar. Viruses enter society by targeting the vulnerable. The vulnerable have fewer resources to protect themselves and fewer choices in terms of where they live or how they access health care and meet their basic needs. While the marginalized bear the brunt of the risk, others are often blind to the consequences of this, failing to see their own role.
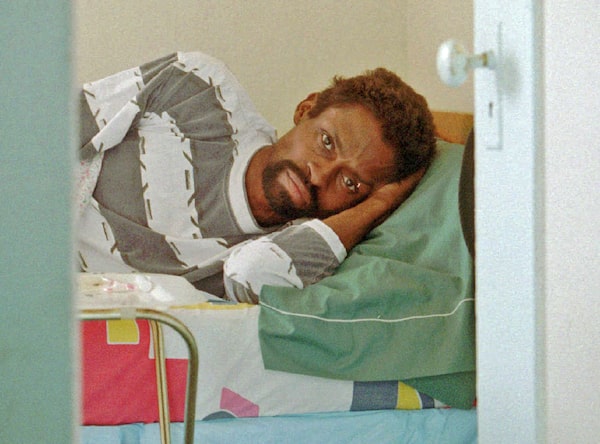
Former Oakland A's and Los Angeles Dodgers outfielder (1972-78), Glenn Burke, lies in his bed at his sister's Oakland, Calif., apartment on Oct. 26, 1994.David Woo-Bloxberg/The Associated Press
The determinants of the spread of viral disease are not merely biological; they are directly related to inequalities in our societies. In this way, COVID-19 is very much following the pattern set by HIV. To ignore the effect of inequalities in the spread of disease will yield disastrous results. Our response therefore has to be swift and our need for resources immediate.
Racism, xenophobia, homophobia, poverty and the devaluation of women all contribute to vulnerability. With those diagnosed with HIV, there was a discriminatory sense that it was “their own fault,” which delayed the support needed to intervene early. Individuals presumed to be infected with COVID-19 will likely fear rejection from others. To compound this, stigmatization prevents those affected from feeling comfortable accessing care. Without addressing the fundamental drivers of the spread of infectious diseases, we will fail to act in time to prevent many deaths from COVID-19.
On the other hand, COVID-19 is different than HIV in many ways. The course of illness is weeks rather than years. It is easily transmitted in day-to-day life. Many of those infected will have a mild illness, but this virus already causes more severe illness in distinct populations, such as the elderly, those with underlying medical conditions and those unable to comply with physical distancing. Quarantine was unhelpful and in fact harmful in the fight against HIV. In contrast, isolation and distancing are necessary to slow the spread of COVID-19. This is the same approach that was implemented to combat the Spanish flu before vaccines and effective medications became available.
Jonathan Mann, the former head of the World Health Organization’s Global AIDS Program, changed the discourse around HIV with his belief that what fuelled that epidemic was discrimination, marginalization, inequitable access to care and a resistance to unify and commit to a global common goal. He believed that without addressing the underlying social conditions, without consistent and co-ordinated leadership, we could not mobilize an effective response to an evolving epidemic. In his words, “What we are doing is necessary, but it is not sufficient."

'John,' an HIV positive man, plants a cross at Oppenheimer Park in the heart of Vancouver's downtown Eastside on July 15, 1997.Nick Procaylo/The Canadian Press
We already knew we were vulnerable to the arrival of another devastating infectious disease. In an article from December, 2018, in the American Journal of Epidemiology, the authors point out that “plagues and epidemics have ravaged humanity throughout its existence, often changing the course of history.” They also chillingly point out that “despite improvements since 1918, governments and health care systems remain inadequately prepared for the impact of a 1918-like severe influenza pandemic.” Preparation requires adequate tools and acknowledging how viruses are able to spread rapidly through our communities.
The need for solid scientific information, equitable access to medical care and co-ordinated global leadership cannot afford to wax and wane. The Spanish flu came with a second wave, and we should brace ourselves for the next surge of COVID-19 when we relax physical-distancing measures. We need sufficient surveillance systems, not just locally but also in developing countries, for any approach to succeed. Otherwise, we’ll be working in the dark.
We cannot limit our options or waver in our focus when tackling a virus. We need to address how this virus has managed to spread rapidly into even remote regions. We need to develop and appoint the kind of leadership in health that is critical to mounting an effective response. We need to empower our communities with knowledge and goodwill. It was the coming together of those at risk of HIV that turned the epidemic around. This time, the at-risk population is almost everyone.

Anne Daniel, left, hugs her son Philip Krstulich, 7, right, as they look over 'Paper Prayers,' an annual exhibition that recognizes those living with AIDS and HIV and commemorates those who have died from the disease, at the Canadian Museum of Civilization in Hull, Que., on Nov. 29, 1998.REUTERS
Over the past 30-plus years, many successes have been achieved in the fight against HIV. We can now successfully treat those infected with HIV, achieving an undetectable level of virus in the blood. In doing so, we can make HIV untransmissible even when having condomless, intimate sex. HIV-infected men and women can choose to have a family without guilt and live productive, valued lives.
In managing HIV care, I have worked alongside the most compassionate and brightest of physicians, many of whom have become lifelong friends to me. They and many others in health care and in the community have been instrumental in changing and valuing the lives of HIV-infected men and women, an achievement made possible only with the sharing of diverse minds and experiences. They are already part of the battle against COVID-19.
Dr. Mann declared that “against AIDS, we will prevail together, for we will refuse to be split, or to cast into the shadows those persons, groups and nations that are affected.” These words can serve as a guide to our approach to fighting COVID-19. Indeed, when WHO director general Tedros Adhanom Ghebreyesus responded to Mr. Trump’s funding-cut announcement, he channelled the spirit of Dr. Mann: “This is a time for all of us to be united in our common struggle against a common threat, a dangerous enemy," he said. "When we’re divided, the virus exploits the cracks between us.”
Through all my experiences, I have come to understand that each person deserves to be seen as a dignified human being with rights and autonomy. We have lessons from our experience with HIV that can prepare us for the battle against COVID-19. Our greatest weapon in the war we are about to fight will be a commitment to creating a responsible and caring society.

People remember the lives lost to AIDS during a minute of silence at a candlelight vigil at the Sixteenth International AIDS conference in Toronto on Aug. 17, 2006.J.P. MOCZULSKI/Reuters
Keep your Opinions sharp and informed. Get the Opinion newsletter. Sign up today.