
The shortage of doctors and nurses in Canada by the end of the 1990s marked the beginning of hallway medicine and long surgery backlogs, which has continued to this day.The Canadian Press
At 10 a.m. on Feb. 14, the hallways of Hamilton General Hospital echoed with a cascade of pings as cellphones lit up with a breaking news alert.
The Ontario government had just announced it would be ending many of its most impactful public-health measures in two weeks, including the vaccine passport system. Dr. Sunjay Sharma, the hospital’s medical director of critical care, was working in the third-floor intensive-care unit when the news broke. As he looked out at the tired staff, dread gripped his chest.
“People are burnt to a crisp,” he said in an interview that day. “We are already having difficulty because of staffing-related capacity issues. We’re being asked to ramp surgeries back up … And then to also say we’re going to take away all of the risk-mitigation strategies?”
With each COVID-19 infection spike the province has seen, Hamilton has been disproportionately pummelled. During the Delta variant wave last year, Dr. Sharma’s ICU was treating nearly twice as many patients as there were official beds. In the post-holiday Omicron surge, the city once again emerged as an epicentre. The strain on a hospital doesn’t just come from the additional patients. Health-care workers are also catching the virus, further depleting already slim staff numbers. (On Jan. 15, Hamilton’s wider hospital network – which includes Hamilton General – recorded 761 staff and physicians in self-isolation, the highest number of absences it’s had during the pandemic.) To cope, hospitals have had to intermittently cancel non-emergency surgeries and treatments, the repercussions of which will be felt for years.
Back in February, some Hamilton nurses warned management they would quit if there was another spike. That moment may be upon us. Fuelled by a potentially more contagious subvariant of Omicron, BA. 2, lighter public-health measures and people taking a more relaxed attitude to the pandemic, the sixth wave appears imminent if not already here. Waste-water surveillance in Ontario, Alberta, British Columbia and Saskatchewan shows infections are climbing once again. In Quebec, hospitalizations are also on the rise.
At the same time, Canadians have grown frustrated with public-health measures. In a January poll from the Angus Reid Institute, more than half of the respondents said it was time to remove restrictions, which provinces have done to varying degrees, scrapping vaccine-passport programs, mandatory masking rules and public-gathering restrictions.
While it may seem hard to believe that hospital staff are still worried about COVID-19 overwhelming their facilities, given that 85 per cent of the eligible population is fully vaccinated – they are.
Long before the pandemic, Canadian hospitals were regularly operating at or above full capacity. Hallway medicine, lengthy surgery backlogs and emergency-room wait times, the shortage of nurses and primary-care physicians, the looming catastrophe in long-term care – these have been top-of-mind problems for more than 20 years. So while only a small fraction of COVID-19 sufferers become sick enough to require hospitalization, Canadian hospitals have had little ability to absorb them, forcing politicians to impose some of the strictest lockdowns and public-health measures in the world.
When the pandemic finally ends, that capacity crisis will still be here, and, in fact, it’s expected to worsen. By 2031, the youngest baby boomers will have turned 65. Life-expectancy rates have been climbing and more people are living with chronic illnesses.
The fix isn’t just adding more staff or building more hospitals, say dozens of experts interviewed by The Globe and Mail. It’s about how the system is organized and paid for. Bed shortages are a symptom of more fundamental ills. To solve the country’s capacity problem, experts say, leaders need to finally confront the deeper flaws in how Canadian health care is structured.

Long before the pandemic, Canadian hospitals were regularly operating at or above full capacity. At Humber River Hospital in Toronto, the surge of patients hospitalized with COVID-19 has only increased the stress on the institution.CARLOS OSORIO/Reuters
“The problem with the Canadian health-care system is that it’s not a system, it’s a collection of dozens of different systems,” said Srinivas Murthy, a pediatric critical-care physician in British Columbia and co-chair of the World Health Organization’s clinical-research committee on COVID-19.
Health care is a provincial responsibility, so Canada has 13 provincial and territorial models. All together, the country spent $267-billion on health care in 2019, before the pandemic. Last year, it was $308-billion, according to new figures provided to The Globe by the Canadian Institute for Health Information (CIHI).
Within each of these 13 models, there are hospital-based systems and regional systems. There are pharmacy-care systems, primary-care systems, long-term care systems, Dr. Murthy explains. To different degrees, they each operate with their own staff, budgets and management structures.
“What that produces is an inefficient level of operations that doesn’t always get the best possible public-health outcomes,” Dr. Murthy said.
The funding model is fractured, too. Most doctors don’t work for hospitals. They are independent, small-business owners who invoice the government based on the patients that they see. Hospital funding is complex and varied, but generally speaking, they aren’t funded on volume like doctors. Notably, no one is compensated for keeping the population healthy, and incentives for higher-quality care or better patient outcomes range from non-existent to weak.
Dr. David Naylor, who chaired the most recent government-sponsored examination of Canadian health care in 2015 as well as the National Advisory Committee on SARS, said the country is in a moment right now, where true change may be possible.
“The worst thing we could do would be to walk away from this pandemic and not understand that it has been a stress test for the health-care system in general – and it’s not fared that well,” said Dr. Naylor.
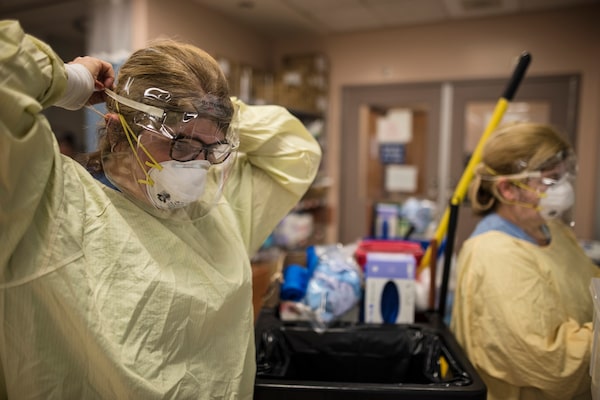
Health care staff don personal protective equipment at North York General Hospital in early March 2020, in preparation for the rising COVID-19 case count in Canada – what would become the first wave of the pandemic.Tijana Martin/The Globe and Mail
In the second week of December 2019, when it is believed the first COVID-19 cases surfaced in Wuhan, China, hospitals across Canada were already strained. The acute-care capacity in British Columbia was 95.6 per cent, Ontario’s was 98 per cent and Alberta’s was 93 per cent at its major hospitals. In Quebec, total bed capacity was 90.9 per cent. Two dozen critical-care physicians working in seven different provinces told The Globe that their ICUs regularly ran at – or over – capacity during non-pandemic times. (Dr. Sharma said 95 to 100 per cent was normal for Hamilton General, pre-pandemic.)
Ideally, intensive-care units are only 80 per cent full, which strikes a balance between efficiency and flexibility, said Robert Fowler, a physician at Toronto’s Sunnybrook Hospital and the chair of the research organization the Canadian Critical Care Trials Group. But maintaining that extra space is expensive.
Capacity isn’t just about a physical bed. It also factors in the personnel required to staff that bed. Years ago, cash-strapped hospitals cut beds as a way to save on head count. Those cuts left Canada with hospital capacity that ranks among the lowest in the developed world.
As of 2019, Canada had just 1.97 acute care beds per 1,000 people, data from the Organization for Economic Co-operation and Development shows. Compare that to Spain (2.48), Italy (2.6), France (3) and Germany (5.95), or the United States, which had 2.46 beds in 2018.
Canada has done relatively well at preventing COVID-19 deaths – all of the above countries have fared worse – but Canadians, particularly those in Ontario and Quebec, have also lived with some of the world’s most stringent and prolonged public-health measures, the Oxford Coronavirus Government Response Tracker shows.

Comparing health care system
performances in 2021
The Commonwealth Fund, a think tank, ranked and
scored the overall performance of 11 high-income
countries’ health care systems based on access to care,
care process, efficiency, equity and outcomes. Canada r
anked second-to-last, ahead of the United States.
Higher performing
Lower performing
Norway
Neth.
Australia
Britain
Germany
N. Zeal.
Sweden
France
Switz.
Canada
U.S.
the globe and mail
Source: the commonwealth fund

Comparing health care system performances, 2021
The Commonwealth Fund, a think tank, ranked and
scored the overall performance of 11 high-income
countries’ health care systems based on access to care,
care process, efficiency, equity and outcomes. Canada
ranked second-to-last, ahead of the United States.
Lower performing
Higher performing
Norway
Neth.
Australia
Britain
Germany
N. Zeal.
Sweden
France
Switz.
Canada
U.S.
the globe and mail, Source: the commonwealth fund

Comparing health care system performances in 2021
The Commonwealth Fund, a think tank, ranked and scored the overall performance of 11 high-income
countries’ health care systems based on access to care, care process, efficiency, equity and outcomes.
Canada ranked second-to-last, ahead of the United States.
Higher
performing
Top 3 avg.
10-country avg.
Lower
performing
Norway
Neth.
Australia
Ger.
N. Zeal.
France
Switz.
U.S.
Britain
Sweden
Canada
the globe and mail, Source: the commonwealth fund
Health professionals told Canadians that restrictions were needed to protect hospitals, even though Canada’s per capita hospitalization rates have mostly been lower than those in Britain, the United States and France.
The truth is: Our hospitals were more vulnerable, because the overall system doesn’t work that well.
Last year, the U.S.-based Commonwealth Fund analyzed the health-care system performance of 11 high-income countries. Canada ranked second to last (ahead of only the United States), because of a poor showing in areas such as access to care, equity and health outcomes.
A lack of funding isn’t the reason for our poor performance. Before the pandemic, Canada spent about 12 per cent of its GDP on health care, which is in line with other universal systems. Canadians are just getting less value for those dollars, says Dr. Murthy.
“I think the austerity over the past 30 years has caused a huge number of problems that COVID-19 has brought to the forefront … so I think we need to spend more money on health care,” Dr. Murthy said. “But investments need to be spent well, and right now, the system isn’t doing that.”
To understand why, Dr. Murthy said, you’ve got to go back to the beginning.
HOW WE GOT HERE
Tommy Douglas and his NDP government enacted the first universal hospital insurance program in North America in 1947, which laid the groundwork for national medicare.Boris Spremo/The Globe and Mail
As the famous story goes, when Tommy Douglas was a young boy, he cut his knee and developed a severe bone infection. His family couldn’t afford the necessary medical treatment, so doctors believed the leg would need to be amputated. But then a sympathetic surgeon offered to operate for free, provided medical students could observe.
That boy grew up to become the premier of Saskatchewan, and in 1947, his government enacted the first universal hospital insurance program in North America. This program, which was later expanded to include doctor’s services outside of hospitals, laid the groundwork for national medicare.
The attachment that Canadians feel toward Mr. Douglas, the mythology around Canada’s universal system and the way it has become politicized as a result is one of the biggest impediments to progress, many experts say. Canadians are so invested in the story they are willing to ignore the pitfalls.
“The thing about Canadian health care is it’s so sacred, it’s impossible to challenge. All it takes is one person to say ‘privatization’ – or anything that could suggest a significant change in what we do – and people lose their minds,” said Dr. Michael Gardam, the CEO of Health PEI, which runs the province’s publicly funded health services. “We need to have an honest conversation about health care … If you don’t challenge something you don’t innovate.”
Step 1, he says, is to critically examine the system that Mr. Douglas – and then the federal government – enacted. That system is actually an insurance program.
“We’ve never really had a comprehensive public health-care system in Canada,” said Dan Roberts, an ICU physician with the Health Sciences Centre in Winnipeg and a former long-time head of critical-care services in that city. “What we have is a scheme that guarantees payment to physicians from public funds. That has nothing to do with having a public health-care system.”
Medicare’s focus wasn’t keeping the population healthy and out of hospital. What it did, in creating a system where the final bill gets paid, but where none of the components are integrated or able to work together, is set up a dynamic for waste and poor care, critics say.
This is why, pre-pandemic, one in six Ontario hospital beds were occupied with “Alternate Level Care” patients, typically elderly people, who no longer need to be in a hospital, but who can’t leave because they still need some care.
Keeping these people in a hospital, rather than finding a way to get them help at home or a spot in a care facility, is worse for the patient and more expensive for taxpayers. It costs the province $500 a day to treat an ALC patient in hospital, $150 per day if they’re in long-term care, and even less if they can be helped at home, says a 2019 report from the Ontario Hospital Association.
Even within individual organizations, such as a hospital, health-care providers aren’t thinking about the money.
In the privatized American system, where the bill goes to an insurance company, every minute of care, dose of medicine and blood test is tracked. As a result, the financial drivers are completely different. For example, in Canada’s public system, ICU beds are a massive expense for hospitals. But in the U.S., they are huge revenue generators, which incentivizes hospitals to add intensive care beds (even if the patient loads don’t necessarily warrant them). This is why the U.S. has so much more ICU capacity: 25.8 beds per 100,000 residents compared to 12.9 in Canada.
This process comes with drawbacks, notably that money, not medicine, can dictate care, but one positive by-product is that the health-care providers know how much everything costs. Some Canadian physicians said they would welcome more financial transparency.
“It’s like going to the grocery store and you have $100, but there’s no price tags. You’re going to bust,” said Joseph Dahine, an intensive-care doctor in Quebec. “If you have no idea of the cost, you know you’re going to make some decisions that are more costly.”
Dr. Dahine said no clinician is going to choose a path that is worse for the patient, but if there are multiple options that are equally good – say different types of medicines – and one happens to be five times more expensive, it makes sense to go with the more economical choice.
The combined effect of these factors – the decision not to invest in preventative care, the lack of system integration and poor financial transparency – made it almost inevitable that health-care costs would explode.
In 1975, which is the first year that CIHI has data, Canada spent $12-billion on health care, or seven per cent of GDP. By 1990, it was $61-billion and about nine per cent of GDP.
Fearing a looming economic crisis, Canada’s deputy health ministers asked medical research professors Morris Barer and Greg Stoddart to examine physician-resource policy. In 1991, the pair’s report concluded that Canada had too many doctors. They recommended a nearly 10 per cent reduction in the number of students being admitted to medical schools and encouraged governments to find ways to limit payments to current physicians, such as setting income limits for specialists. Barer and Stoddart’s findings fed into a prevailing concern at the time that health-care spending was out of control.
Having struggled through the recessions of the early 1980s and 1990s, the federal government was taking on more and more debt. It began reducing transfer payments. The provinces responded with sweeping cuts to health care, from bed capacity to personnel.
In Ontario, NDP Premier Bob Rae put a cap on medical-school enrolments. In Nova Scotia, doctors saw their fees reduced by 18 per cent owing to policies passed under Liberal Premier John Savage. American recruiters moved in and many doctors left the country. In Alberta, Conservative Premier Ralph Klein cut the province’s health-care budget by nearly 20 per cent.
Dr. Noel Gibney, who held a leadership role with Edmonton’s health authority during the cuts, said his city lost 25 per cent of its ICU capacity. Those beds were eventually brought back and more were added, but “as the pandemic showed – nowhere near enough.”
Dr. Kusum Menon, a pediatric intensivist at the Children’s Hospital of Eastern Ontario in Ottawa, says that when she started working at CHEO 30 years ago, there were about 350 hospital beds. Today there are 134.
During this period of cuts, thousands of full-time nurses in Canada lost their jobs. It became common for hospitals to hire nurses on contracts or as part-time staff. New hires have never kept pace with population growth since then. In 1991, CIHI data shows that there were 937 registered nurses per 100,000 people in Canada. Just before the pandemic, it was 800.
By the end of the 1990s, Canada was grappling with a shortage of doctors and nurses. This was the beginning of hallway medicine and long surgery backlogs.
The extent of how bad things had gotten was very publicly revealed in 2000 when the World Health Organization published a report ranking the Canadian health-care system 30th in the world. Julio Frenk, one of the authors, told The Globe at the time that a primary reason for Canada’s poor showing was the lack of efficiency. His study determined that 12 cents of every dollar spent was being wasted.
It was an international embarrassment and in quick succession, two massive reviews came out of Ottawa, the Kirby Report and Romanow Commission. Between the two of them, the reports called for a variety of reforms, including more money to the provinces, changes to primary care, more medical and nursing students and more focus on preventing illness and injury. Other high-profile reports have come out since.
“It’s always the same solutions,” Dr. Dahine said. “But they’re only ever partly implemented. And they’re almost always implemented on top of things we’re already doing. It’s never less to do or do things differently.”
As a result, these cherry-picked fixes have been layered onto a crumbling foundation that Canadians have collectively been ignoring.
And then came COVID-19.
THE SOLUTIONS
During the Omicron wave in January, the hospital network that oversees Brampton Civic Hospital declared the rarely used “Code Orange.” This is typically used to signify that an unforeseen disaster is under way. The move was triggered because demand at the hospital had dangerously outpaced capacity.
Brampton, which is just outside of Toronto, is the country’s fastest growing large city. Not coincidentally, the region’s hospitals, which were overflowing before the pandemic, have been battered these past two years. (Brampton Civic’s emergency department was designed to handle 90,000 patients annually, but it was averaging 130,000 pre-COVID-19.)

Health care workers attend to an ICU patient at Brampton Civic Hospital. The region’s hospitals, which were overflowing before the pandemic, have been battered by the past two years of the pandemic.Fred Lum/the Globe and Mail
This was the backdrop that Ontario Premier Doug Ford chose on March 15 to announce that his government would be adding more than 450 spots to the province’s six medical schools. Earlier in the month, his government agreed to pay eligible nurses a retention bonus of $5,000. Other provinces are taking similar steps to deal with staff shortages, which health experts agree is Priority 1 in order to survive the next few years.
In Alberta, nurses recently won a 4.25 per cent pay bump as part of a new collective agreement that included a one per cent lump-sum bonus. Last September, Quebec Premier François Legault announced eligible full-time nurses would receive a one-time payment of at least $15,000. Any nurse who had quit or retired would be given $12,000 if they came back to the public system. From British Columbia to New Brunswick, nurses are being offered signing bonuses.
Some hospitals have also looked at adding “extenders” to nursing teams. These are people who may or may not be regulated health workers, who could assist with simple tasks, such as bathing or feeding a patient. The extender strategy is aimed at addressing the immediate staff crisis. But it’s this type of thinking – re-examining who does what and finding efficiencies that also make the system run better – that reform advocates are pushing for.
In interviews with The Globe, doctors raised dozens of suggestions to modernize and improve Canadian health care. Some were specific to their institution, but the big-picture ideas typically fell in one of four buckets: integrate the silos, adjust the funding model, better utilize data and performance indicators and start a conversation about how private dollars could be leveraged to improve the public system.
At Hamilton General, Dr. Sharma says when people hear the “the p word” they think of the “free-for-all” American system, which derails any discussion about how private investment could ease some of the strain in Canada.

The UK's National Health Service (NHS) has universal coverage and non-public options, including about 500 private hospitals that offer specialized services.HENRY NICHOLLS/Reuters
“There are other Commonwealth countries with robust public health care [and] a private system that’s properly regulated … that still maintain equity and access,” Dr. Sharma said. He pointed to Australia as an example, a country that has scored higher than Canada in health-care rankings. The United Kingdom also has universal coverage and non-public options, including about 500 private hospitals that offer services such as cancer screening, colonoscopies, fertility treatments and bariatric surgery.
About 30 per cent of Canadian care is already privately funded. Mental-health services outside of hospitals, for example, are typically paid for out-of-pocket. As is dentistry, optometry, prescription drugs and physiotherapy. More than half of Canada’s nursing homes are privately owned.
Experts who are interested in exploring more privatization say Canada could look at incorporating more specialized facilities, such as the Shouldice clinic in the Toronto area, which exclusively does hernia repair. Shouldice is one of the only for-profit hospitals in Canada, although most of its work is done on contract with the Ontario government.
Privatization was the one area that generated strong opinions – for and against – among the doctors who spoke to The Globe. Some preferred that Canada focus on pulling more uninsured services under the public umbrella. (This may happen. NDP Leader Jagmeet Singh and Prime Minister Justin Trudeau recently announced a power-sharing deal that would see the federal government introduce an income-based dental-care program and universal pharmacare.)
Where there was consensus was the need to break down the silos.
Integration was a central theme to the 2015 “Unleashing Innovation: Excellent Healthcare for Canada” report, Dr. Naylor’s analysis for the federal government.
To highlight the absurdity of the status quo, it poses a hypothetical example of a person who had been seriously injured in a car crash. This patient would need acute care in a hospital, and then rehabilitation, home care, outpatient physical and occupational therapy and drugs. They may also need dental services, psychological counselling and assistive devices.

The ideas doctors raised in thinking about how to modernize and improve Canadian health care typically fell in one of four buckets: integrate the silos, adjust the funding model, better utilize data and performance indicators and discuss how private dollars could be leveraged to improve the public system.CARLOS OSORIO/Reuters
“Care for this citizen would involve tapping into a dozen separate private and public programs … Such a patchwork can hardly operate in the best interests of the patient and his or her family,” it reads.
This lack of integration contributes to the dysfunctional way in which health care is funded.
Right now, physicians and hospitals are paid using different budgets, creating a myriad of problems, including that physicians are not rewarded for being effective team members, for innovating, for being leaders or good stewards of public money. And they’re not compensated for providing better care.
Dr. Naylor said Canada’s regional nature means one system isn’t going to work everywhere, but in a post-COVID-19 world, some “intelligent experiments” with different models should be done. The result doesn’t mean doctors need to make less money – Canada wants its physicians to stay in this country – but incentives should be aligned.
He is particularly interested in a bundled model system. Imagine a scenario, he explains, where a person needs a hip replacement and the government provides a single envelope of money to manage every step of that process – the doctor’s fees, the surgery itself, medications, outpatient therapy, etc. If any savings are found along the way, that money stays with the institution.
“What happens is that you then create a positive incentive to reduce the overall cost of care and to maximize the outcomes,” he said. Because the flip side is that if there is a complication and the patient needs to be hospitalized again, there’s no extra money.
(In this system, health-care funders would account for the fact that a certain percentage of cases will be more complex, but that extra cost would be built-in, similar to how insurance policies spread risks across large numbers of individuals.)
Kevin Smith, the president of the University Health Network in Toronto, has implemented small-scale versions of bundled payments at UHN as well as at St. Joseph Health System in Hamilton, where he used to work. At St. Joseph’s, the hospital co-ordinated with long-term care and home care to provide one seamless continuum. Patients encountered the same staff, regardless of where they were being treated, and the staff could take better care of the patients because they didn’t always have to hand them off to new people, Dr. Smith explained.
“In this [bundled model], money follows the needs of the patient. Where is the best place for the patient to receive this care and in a system that is economically restrained,” Dr. Smith said.
Jason Sutherland, an internationally recognized expert on health-care funding, is a fan of this method, particularly as it incentivizes better care. In fact, he would like to see a funding model in Canada that ties hospital budgets to patient outcomes.
“I push this all the time. It’s whether I can get people to listen,” said Mr. Sutherland, who in addition to being a professor at the University of British Columbia, helps multiple provincial governments in Canada as well as in the United States evaluate their hospital funding models. In the United States, there are entities such as Accountable Care Organizations (ACOs) that document and analyze patient outcomes.
In all of Canada, Mr. Sutherland only knows of one jurisdiction that tracks how patients do after surgery: it’s the program that he started in Vancouver nine years ago with the support of the local health authority and a grant from the Canadian Institutes of Health Research.

While only a small fraction of COVID-19 sufferers become sick enough to require hospitalization, Canadian hospitals have had little ability to absorb them.Graham Hughes/The Canadian Press
Six hospitals are involved and they focus on eight surgical specialties, he said. Patients who are scheduled for surgery are identified and then their health and symptoms are measured before and after their procedure. The program has helped clinicians flag issues such as the fact that depression can be a major problem for those on surgery wait-lists and if untreated, it seems to coincide with worse outcomes. Now, health providers know to look out for this and get patients help. It’s also been a resource for surgeons to monitor their performance.
“I am very frustrated with the way that provincial ministries of health just act as a paymaster. You know, you are also responsible for all of your residents’ health. You must measure it to improve it,” he said.
The lack of performance indicators in Canadian health care was a complaint raised by many experts, as was the lack of data in general.
Elyse Berger Pelletier is an ER physician who, until last fall, was the deputy director general of emergencies and EMS in Quebec. Through that role, she led an initiative aimed at modernizing and streamlining the province’s emergency rooms.
During the second COVID-19 wave, the ministry became aware of an urban hospital that was struggling, she said. When her staff looked at the numbers, they noticed the hospital was admitting five to 10 per cent more patients than others in the region, despite similar patient demographics and level of disease in the community. This was a signal that some of those admissions may not have been necessary.
The ministry and hospital administrators then looked at other bed usage statistics. There is nationally available data that shows the average length of hospital stay for various procedures. This hospital was keeping patients longer than average in many cases. By making some length-of-stay adjustments, the hospital freed up enough beds to weather the wave.
“If you go into a U.S. hospital for a pulmonary disease … the doctors know you have to stay – I’m making this up – three days. The insurance company is going to pay for three days. Everyone knows. In Quebec, ask the doctor what is the average length for pulmonary disease, they have no clue … we aren’t trained like that,” she said.
Some Canadian jurisdictions are better at this than others, Dr. Berger Pelletier added, but in general, leveraging data could do a lot to free up capacity in the short term.
It’s a solution that’s just sitting there, she said, if only leaders will act on it.
Two weeks ago – a few days before Ontario was scheduled to drop most of its mask mandates, one of the province’s few remaining restrictions – a Globe reporter contacted Dr. Sharma to see how things were going at Hamilton General. Were they seeing more cases? How was the staff? When he didn’t phone back, the reporter tried text message.
Many hours later, Dr. Sharma finally replied: “Sorry. Got COVID and sick as a dog.”
Our Morning Update and Evening Update newsletters are written by Globe editors, giving you a concise summary of the day’s most important headlines. Sign up today.
 Robyn Doolittle
Robyn Doolittle Tom Cardoso
Tom Cardoso